PART 2: What’s it like doing CBL?
20 March 2020
So last blog, we talked about how PCS (the first term) was so important to build the foundations for CBL = case based learning. This blog, I will talk about how it works and share some more quotes about it!

So how is CBL organised?
CBL is spread over Year 1 & 2 with 17 cases overall – 6 of which are completed in Year 1. Each case lasts for 2 weeks and there is a similar timetable for each case, as shown below. You either have a morning or an afternoon case group. This will determine which day your weekly placement will be on (Tuesday or Thursday) – to be discussed in Part 3!
Case groups are usually around a group of 10 with a facilitator, which can be staff from C4ME (centre for medical education) or clinicians. This is why PCS tutorials are a great transition because you already have experience of SGL. You get to meet your case group at the end of PCS to do a practice case to find a system that suits you, which I will explain further later on and you are with them for the rest of the year.
You also have different case groups in Year 2 for first and second term which has been great to meet new people on a smaller scale. It sounds silly but because the year is so big, there will be some people you will never even notice and if it wasn’t because of case, you wouldn’t get to know them so it’s great for mixing as well!
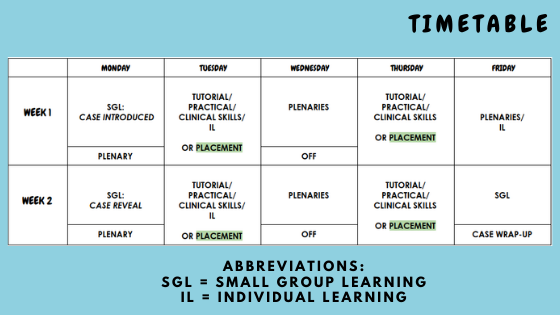

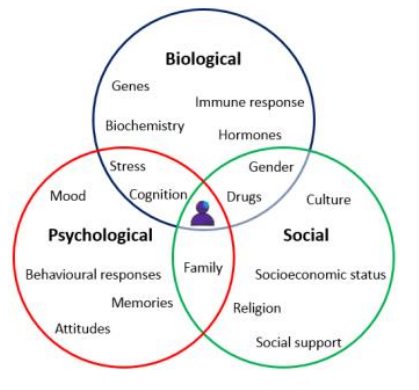
Week 1: Day 1 – the case scenario is introduced! What’s great is that they are all based on real life patient cases and developed to ensure that as a group we look at the patient holistically, looking at the 3 factors shown in the Venn diagram.
As a group, you will define terminology that you don’t know. For example, this could be a name of a drug which all allow you to explore the pharmacological management of the patient or perhaps a name of a secondary care service to help appreciate all bodies involved in the patient’s care. Having identified all the factors, you work through each one and talk about what you already know drawing on your knowledge from PCS and other related cases. This helps to identify gaps in your learning, for which by the end of the session you form learning outcomes to go away and research. The role of the facilitator is to ensure that you do not go off track in discussion and ensure key points have been covered. They may prompt or offer some anecdotes from their personal experiences, but the point is that it is a peer-led discussion.

This is set up that each session there is always a chair and a scribe. When you meet for your practice case, usually a rota is formed so that everyone gets a chance to lead, but often the most important part of the rota, as Kane has mentioned, is the cake! After all we all know that CBL really stands for CAKE BASED LEARNING! Quite often it will be treats from Tesco Express easily picked up right outside Taly!
So you’ve made learning outcomes: how do you get the information to achieve understanding these?
Your individual learning (often referred to as SDL = self-directed learning) is guided from plenaries and other sessions in the week which surround the topic of the case, as well as your own research from textbooks and websites. In this way, your learning is very structured but stems from a patient centred context which is a value that will continue throughout your career.
What’s great about the second session is that you come back and discuss the information that you have found on all the outcomes. As Millie has perfectly summarised, it’s so important to review the information because this is the time to clarify anything that you didn’t understand from the week and you can help each other to make sure you are all on the same level before moving on!
The next part is the case reveal! This is the second part of the scenario which usually describes developments in the patient’s condition. It is usually shorter because the next session is only a few days later, but the same approach is applied – some more learning outcomes are formed. You then use the different teaching styles provided in the week as well as your own information to come back to discuss on the Friday and discuss thoughts and opinions of the case as a whole.

To complete the case, the case leads (people who wrote the case) deliver a case wrap-up plenary to summarise the whole case, what you should have discovered and often test knowledge with useful quizzes. Sometimes they bring in guests who have relate to the patient case to talk more on the social aspects which is always very interesting and inspiring. At the end of the case, they release the official learning outcomes, which is useful for revision to checklist your learning.
Then the next week, it starts all over again – a new case! There are other weeks slotted into the timetable for example for projects known as SSCs (student selected components), but in general CBL is very enjoyable and when you go back to revise for end of year exams, it’s amazing to see how much you have learnt from it!
Ntuse has picked up on a great point about adapting learning. This is because by the time you get to the end of PCS, you figure out a system that works for you to make notes whether that maybe typing, writing out or a mixture. Then the timetable is different – there is more time to research but you have to make sure you get your notes done in the timeframe to come prepared for the next session. Although you do bring notes, it is encouraged to close laptops/ put away notes at first so that it is a true discussion and you are learning from each other. This is how it differs from PCS tutorials as well.
So finally probably one of the most common questions of all: what makes CBL different to PBL and others?
Honestly, I wish I could explain the difference because it’s not something that even I have fully understood due to the similarities. However, what I can say is from my experience, CBL is very structured and there is a clear direction of what should be achieved by the end of each case. (To my understanding, this is something which is doubted by some PBL courses).
Also, Cardiff is renowned for this teaching and some other medical schools have been inspired to adapt their curriculum like Cardiff so it goes to show how good it is!

I hope I have been able to give you a better insight into CBL and please feel free to ask more questions by commenting below or messaging me on my Unibuddy account. Go back to the intro blog to find the other parts of the subseries!