Get CreActive for Hips – Living with Hip Dysplasia
13 May 2021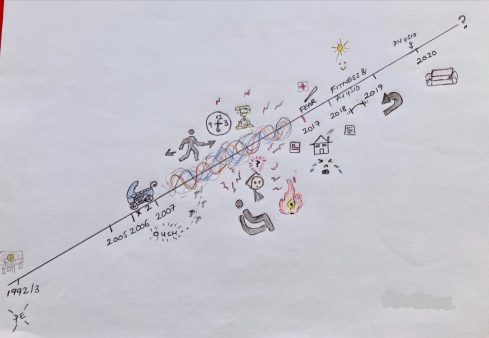
Background
Young adults with acetabular dysplasia (hip dysplasia), an orthopaedic condition of the hip, often undergo multiple surgeries and can experience chronic pain, insomnia and difficulties walking which effects both their physical and mental health. Consulting with young adults with hip dysplasia in a seminar series in 2018, we know that specialist services for them are limited and getting access to advice about pre and post-operative rehabilitation is difficult. Such a lack of specialist servicesand readily available support can leave young adults with hip dysplasia feeling isolated and unsure about what physical activity they can and can’t do. Without connection to a peer support group via local services, this can disempower them further.
Get CreActive
To begin tackling some of these issues, we are working with a group of 20 young adults with hip dysplasia. Through a series of online gatherings and creative arts workshops we are exploring their experiences of living with hip dysplasia, learning about being physically active with this condition and setting research priorities for the future. The project, ‘Get CreActive’ will conclude with the creation of a website displaying shared experiences and key learning from the project which will be used as a resource and a hub for connecting young adults with hip dysplasia to one other. This blog explores the first phase of the project – sharing experiences of living with hip dysplasia.
Women and hip dysplasia
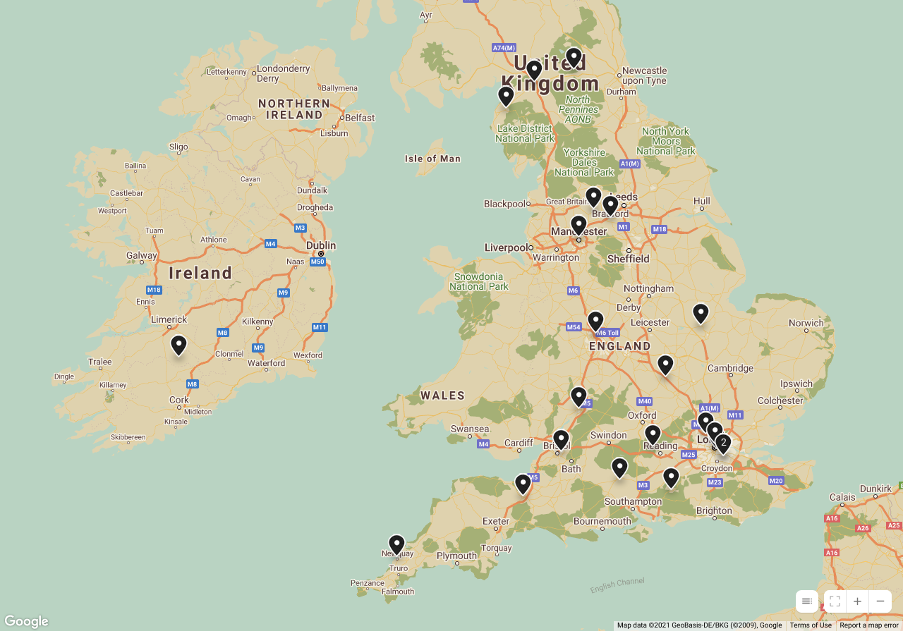
All women, the group range in age from early twenties to early sixties and are spread geographically across England, with one person joining us from the Republic of Ireland. With a range of nationalities represented the group includes people from England, Australia, the Republic of Ireland and the Ukraine. With women outnumbering men with hip dysplasia 10:1 it is no surprise that we attracted only women to the project. Since starting the project however we have made contacts with women whose male partners have hip dysplasia and future work will seek specifically to find and connect men with hip dysplasia.
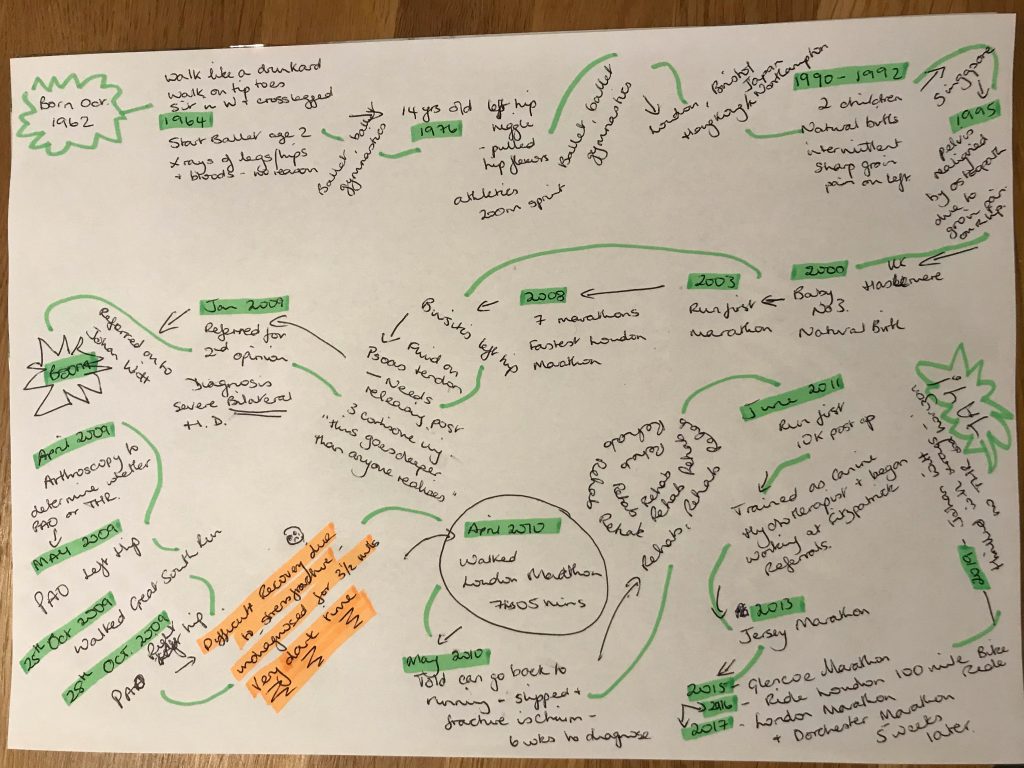
Drawing timelines
We kicked the project off by inviting everyone to draw a timeline charting their life with hip dysplasia. We hoped that the timeline would provide everyone taking part with a frame to talk to when meeting the rest of the group for the first time and being asked to share their experiences. The timelines did just that – eliciting detailed and often emotional narratives about what living with hip dysplasia has been like for them.
For some of the group their timelines didn’t begin until they were in their 30s or even early 40s due to their hip dysplasia going unnoticed – or undiagnosed. For others, their timeline started at birth or early childhood.
A wide range of personal journeys unfolded across the first few sessions as the group met one another and explained their experiences of diagnosis, surgeries, ‘pre-hab’ and rehabilitation. However, despite different starting points, ages, lifestyles etc., their experiences were startlingly similar – and the parity of what they did share, obvious to all.
Diagnosis and treatment challenges
Many of the group had gone years without a diagnosis, their pain without explanation and many had been left feeling not believed by the medical professionals they interacted with. Once diagnosis did come, while the validation of their symptoms provided relief, diagnosis often meant multiple surgeries. These ranged from arthroscopies to pelvic osteotomies – with the pelvic acetabular osteotomy the most common intervention experienced by the group. Designed to preserve the dysplastic hip for as long as possible and pushing the need for a total hip replacement as far into the future as possible, pelvic osteotomies are extensive surgeries with lengthy recovery periods for those receiving them. While they promise the best chance at preservation, they do not promise a pain free or return to presurgical physical abilities.
The rehabilitation journey
However, it was not the post-surgical pain, the months of rehabilitation that follow these surgeries that the group focussed on, but other aspects of their surgical experience which seem to ‘cut the deepest’. For those without family members able or willing to help care for them in the early stages following surgery, care at home was needed. The indignity of needing support to wash, dress and even toilet as a young person is the core memory left for some. For others, visceral aspects of surgery not explained ahead of time were remembered as traumatic by these young adults – including, catheterisation and bowel management; and unasked or unanswered questions about how menstruation might affect surgery added to their anxiety pre-surgery. Coupled with health care professionals not always being familiar with their particular surgery and expecting them to rehabilitate like those with a total hip replacement, many of the group were left to advocate for themselves and educate those they met about the reality of their surgery and their needs.
The group’s timelines were also full of rollercoaster type experiences of recovery post-surgery, noting ups and downs of progress and setbacks, and detailing the repetitive nature of multiple surgery-rehab cycles. Timelines also touched on how hip dysplasia had impacted upon family and friends and on their relationships. In project sessions, while talking through their experiences, group members often reflected on what their parents went through for those whose hip dysplasia had been diagnosed as a child. They wondered what it must have been like for them to have a child going through multiple interventions and surgeries. The impact on and support needed by partners also came out in discussions.
Relationships and post-surgical rehabilitation process
Some of the group reflected how important support from their family had been to them but reflected how many of their friends did not realise the extensiveness of the surgeries they were undergoing and were not as supportive as they had hoped (and needed) them to be. Some reflected that their partners did not know or understand the journey ahead for them and needed support themselves in dealing with the post-surgical rehabilitation process. Others recognised that the chronic nature of their condition and how the pain they experienced effected their mood had strained relationships and contributed to the breakdown of relationships.
Overcoming challenges
They were, however, also full of triumph – stories of succeeding and achieving – reaching fitness milestones or loosening the grip pain had on their lives and well-being. They also told of adaption, of trying new things, setting new goals and included an amazing commitment to being physically active.
In the next blog, we will explore what being active means to the group, the challenges of getting active again post-surgery, what exercise and activities works for them and why.
Dr Julie Latchem-Hastings
Follow @getcreactive for project updates
- February 2026
- December 2025
- October 2025
- June 2025
- May 2025
- April 2025
- March 2025
- February 2025
- December 2024
- November 2024
- October 2024
- September 2024
- July 2024
- June 2024
- May 2024
- April 2024
- March 2024
- December 2023
- November 2023
- September 2023
- July 2023
- June 2023
- April 2023
- March 2023
- February 2023
- December 2022
- November 2022
- October 2022
- September 2022
- August 2022
- July 2022
- June 2022
- May 2022
- April 2022
- March 2022
- February 2022
- January 2022
- November 2021
- September 2021
- July 2021
- June 2021
- May 2021
- March 2021
- February 2021
- December 2020
- November 2020
- September 2020
- August 2020
- July 2020
- January 2020
- December 2019
- October 2019
- September 2019
- July 2019
- June 2019
- May 2019
- April 2019
- February 2019
- December 2018
- November 2018
- October 2018
- September 2018
- August 2018
- July 2018
- June 2018
- May 2018
- April 2018
- March 2018
- December 2017
- October 2017
- August 2017
- July 2017
- June 2017
- May 2017
- April 2017
- March 2017
- February 2017
- January 2017
- December 2016
- October 2016
- August 2016
- June 2016
- April 2016
- March 2016
- February 2016